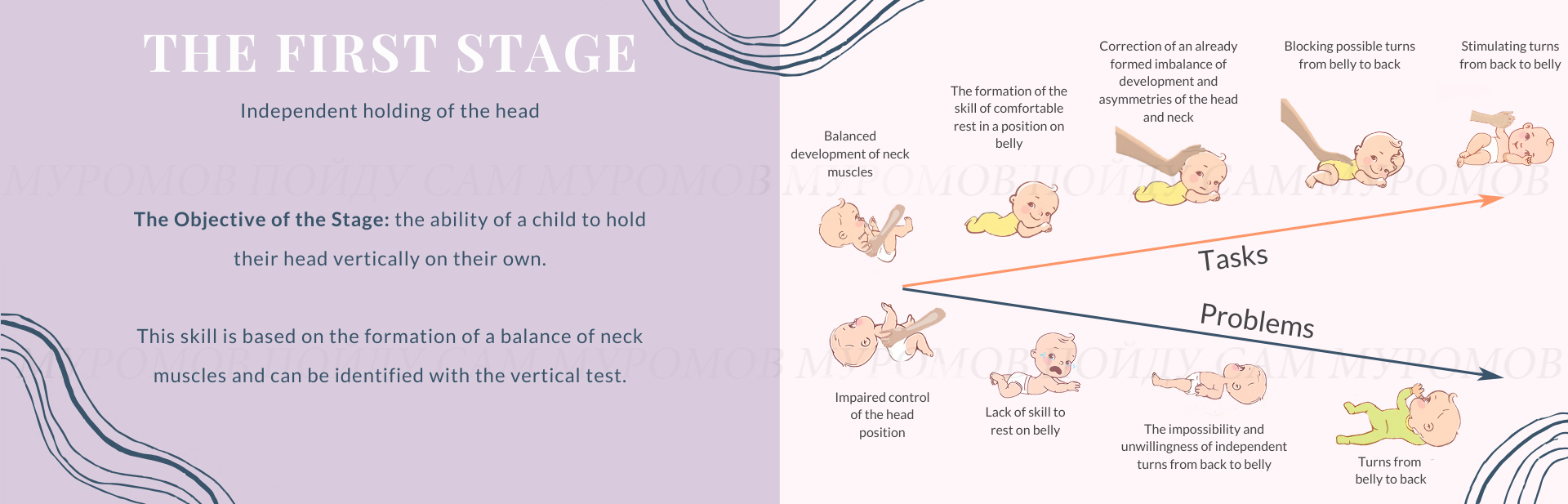
The motor development of the child during the first year of life is rich in events connected with the acquisition of new opportunities: in the fourth month, turns are formed, then army crawling, sitting, standing up on all fours, crawling on all fours, standing up on feet and walking. The child demonstrates new movements and emotions regularly. The first three months of life are not rich in the acquisition of new motor skills. But especially at this time, the foundation of harmony of future movements is laid. In our opinion, the main event of this period is the emergence of the ability to independently keep the head vertically regardless of where the body tilts. This skill is based on the formation of a balance in the work of the neck muscles and is revealed with the help of a vertical test, which we will talk about a little later.

The work of the muscles of the front surface of the neck (sternocleidomastoid)

The muscles of the lateral surface of the neck (left)

The work of the muscles of the lateral surface of the neck (right)

The formation of the skill of comfortable rest in a position on belly.

Correction of an already formed imbalance of development and asymmetries of the head and neck.
In the meantime: how is such a balance formed?
Let us turn to the anatomy and physiology of the neck, the muscles of which provide head movements. Let us divide them conditionally on the muscles of the front surface, the main of which are «sternocleidomastoid» muscles, the muscles of the back surface, and lateral surfaces. The muscles of the front surfaces tilt the head forward, raise it from the supine position. The muscles of the back-surface tilt the head back and raise it from the position on belly. The muscles of the lateral surfaces tilt the head in the appropriate directions.
Normally, the balance of the work of the neck muscles is formed in the first three months of life. It happens gradually and unevenly. Right after birth and up to three months, the muscles of the back surface are more active and functional. It is explained by participating in the protective unconditioned reflex of newborns, which is the ability to lift and turn head to the side while lying on a belly. The activity of the muscles of the front surface of the neck - the sternocleidomastoid - is expressed in the ability to briefly hold the head, not allowing it to tilt back when the body is tilted back, as well as in the ability to hold the head on the back of the head for a while in the supine position. The developing nervous system creates the conditions for their accelerated development, which leads to the possibility of holding the head vertically for two months. It is not easy for these muscles. Their work is complicated by a relatively short neck. Nevertheless, they develop functionally, though there is no full balance. Being able to raise the head and keep it vertically in the position on a belly, the child is not able to do the same thing being in the supine position. Such a possibility appears to the end of the 4th month of life, and it appears by the ability to start the turn from back to belly. The position on a belly is interesting for a child to this moment thanks to previous practice.
Let us emphasize, that it happens this way just normally!
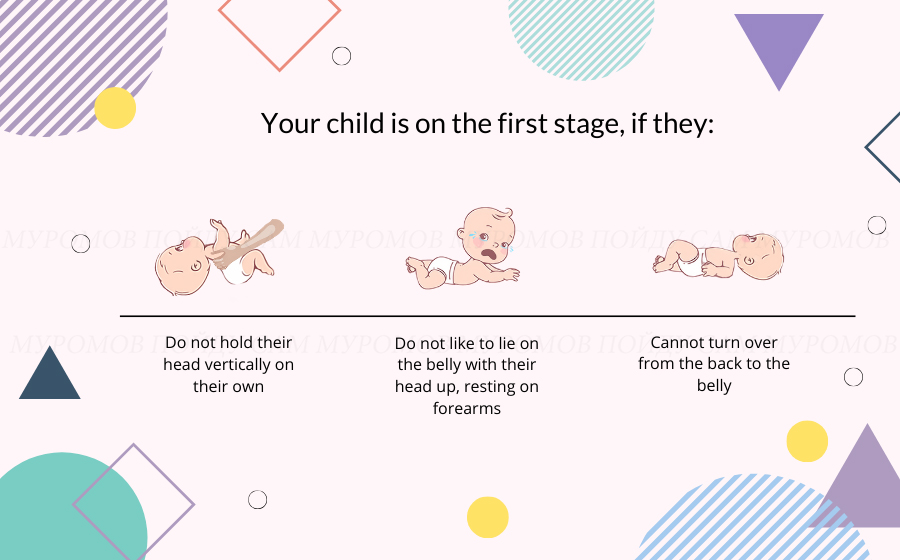
Let's imagine a less positive scenario. With various disturbances of the development of the nervous system (the reasons can be very diverse), the mechanisms of forming the balance of the flexors and extensors are disturbed. In the vast majority of cases, the development of «nods» (sternocleidomastoids) is delayed. As a result, by two months the child does not keep the head in a vertical position (it «falls» back), and, as a result, the formation of turns from back to belly is delayed. Almost always, the imbalance is exacerbated by the action of related factors – the external environment. As already mentioned, these are the «healing» effects and the everyday routine of the child.
Judge for yourself:




With a spiral imbalance, the head in different positions tends to more often or (and) to a greater degree of turn in one direction. With lateral in different positions, the head is more inclined to one shoulder, often involving the muscles of the body on the same side and forming an arc.
Let's return to the vertical test (VT), which is necessary for an additional diagnosis of the condition of the child. It reveals the types of imbalance of the head and neck, their severity and indicates the direction in which you need to start working. It is performed in conditions comfortable for the child when they are calm, full, and do not want to sleep.


If the child responded to these actions by moving the head forward and holding it, then the test is positive (VT +).

If the child, in addition to holding their head, tries to bend their legs, pulling their knees to their belly and significantly straining the abdominal muscles, groans, then the test is brightly positive (VT ++).

If the above-described sensations do not appear, and the head, when leaning back, did not actively stretch forward and (as an option) «fell» due to the deviated support, then the test is negative (VT-).

If the child with all their might rests the back of the head on the chin to the tester even during the vertical position and continues to do so when the body is deflected, the body and legs are unbent, then the test is sharply negative (VT- -).

During the test, it is necessary to control the reality of the deviation back, being sideways to the mirror and peeping into it or asking a third party to evaluate the deviation from the side.
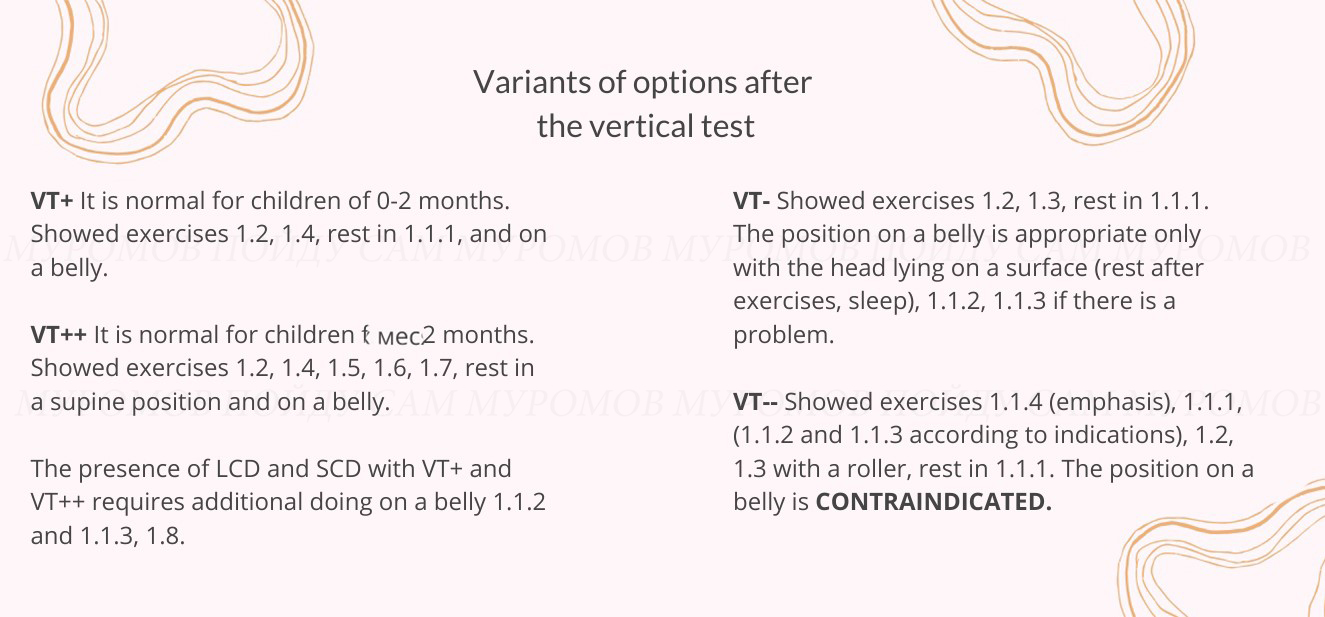
VT + and VT ++ are the norm and say that it is possible and necessary to use in life the active positions of the first stage – 1.3 and 1.4 (see below), the positions on belly can and should be used.
VT- is always an occasion to recheck it many times. If the conditions for the test are met, and they performed correctly, it is necessary to look for a reason, starting from the lethargy of the child after the illness.
VT- - is always a cause for concern. It makes impossible the active positions of the first stage, as well as any kind of being on belly, significantly restricts everyday routine.
During a vertical test, it is possible to identify or suspect lateral and spiral cervical imbalances. These are important findings that need to be clarified using a side inclined test, a rotary test, and monitoring a child lying on their belly and lying on their back.
Lateral cervical imbalance (LCD). With VT +, you can see the head tilt to the side, sometimes very significant. With VT- only significant deviations are detected. Carry out the lateral inclined test after the vertical test in any case and clarify the situation. The lateral cervical imbalance will be confirmed by the difference in the amplitudes of the tilt of the head to the side. When the child in the position on belly, a lateral trunk imbalance is often revealed additionally. The body, along with the head, neck, and legs, takes the form of an arc. A similar pattern may be observed on the back.

Spiral Cervical Imbalance (SCD). When performing a vertical test, you can see that the child turns their head with a larger amplitude in one direction. In the supine and abdominal position, the child also prefers to turn their head in one direction. A mild imbalance can be detected by turning with the child in position 1.3 (see below) in front of the object that interests them. In one direction, the amplitude of the head rotation will be less.

Lateral and spiral cervical imbalances can be marked with VT + and VT-, occur not only in the first stage, and must be checked for any child.
All described disturbances of the development balance of the muscles of the neck can be combined in any combination and are often observed in one child. With a moderate severity of the imbalance, children can master turns on belly, but very often such turns are performed by extending the body and pushing the foot mainly in one direction. With a pronounced imbalance, the child is not able to turn over on their belly, but at the same time, they first fall from belly very quickly, then consciously turns over onto their back.
At the first stage, the presence of turns from belly to back is a sign of impaired development. The vertical test is usually negative or sharply negative. Any stimulation measures in belly are contraindicated: back massage, ball rolling, swimming with a circle, etc.
Significantly less often, turns from belly to back are present against a positive vertical test. The main task in this situation is to completely block such turns.
It happens that the ability and desire to keep the head in the supine position is poorly expressed or absent in children with VT ++. The options for exercise 1.6 will help in the development of this skill (see below).
МA child with VT ++ and the formed skills of resting and holding the head in the supine position most often begins to roll on their belly on their own. We can help them by stimulating turns with exercise 1.7 (see below).
1.1 Layings 1.1.1 - basic, 1.1.2-lateral, 1.1.3-spiral, 1.1.4-paper clip.
1.2 Stimulation of bringing and holding the legs.
1.3 Stimulation of bending and holding the head in a standing position (with and without a roller).
1.4 Stimulation of holding the head half-lying.
1.5 «Monkey» (sitting, standing).
1.6 Stimulation of lifting and holding the head lying on belly.
1.7 Stimulation of turns from back to belly.
1.8 Blocking turns from belly to back.
Runs from a few seconds to several minutes no less than hourly.
The supine position. Head and legs are raised. The chin is pressed to the chest.

Laying for correction of lateral cervical imbalance (LCD). It is performed on the hands or the knees. When the head is tilted to the right, laying is performed on the right side, when tilted to the left on the left.

Laying for the correction of spiral cervical imbalance (SCD). It is performed on flat surfaces with fixation of the head and pelvis. The head is fixed by the face in the direction opposite to the deviation. This laying can be done while sleeping, turning the child's head in the right direction.




Laying is done in two ways. In the supine position on the parent’s lap, the soles of the foot are brought to the head and fixed. The chin is pressed to the sternum. In a position on the surface, the head is pressed against their forehead.




All variants of this stimulation are performed in the supine position with the head pressed with the chin to the chest and are offered with increasing complexity. The objective of this exercise is to independently hold the child's legs, knees brought to belly. If the task is not performed with the help of light exercises, then we use more complex ones. All methods of stimulation are divided into massage effects on the anterior abdominal wall, anterior surface of the thighs, and effects on the foot (feet) with objects with an irritating effect.






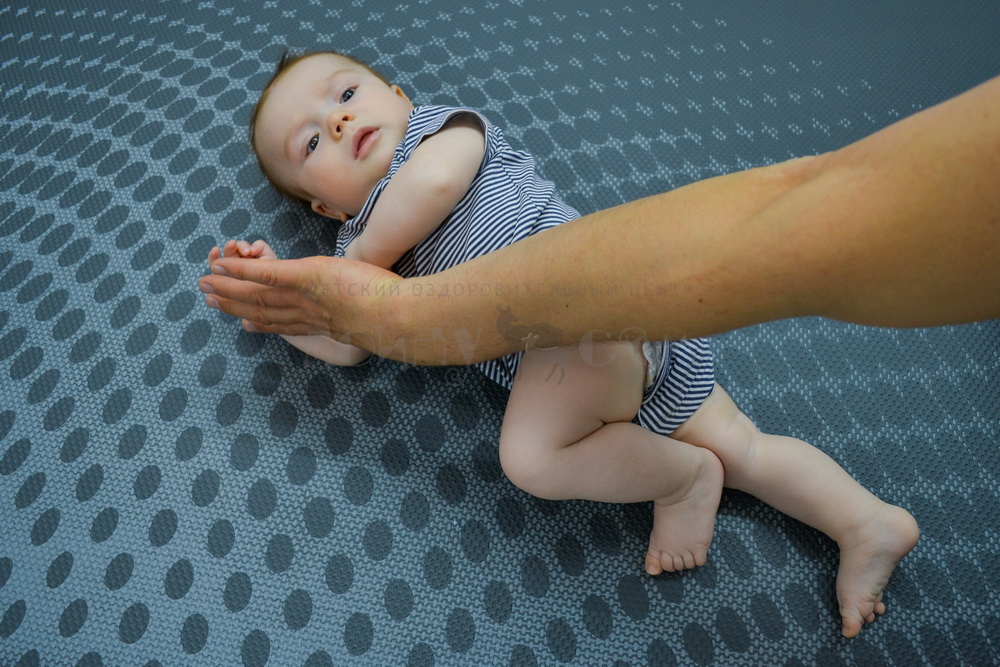
Exercise is a way of holding a child well, being a continuation of the vertical test. With VT + and VT ++ it is performed without a roller; with VT- and VT-- it is performed with a roller under the head. Exercise is effective only if there is a deviation of the child’s body back, which is achieved by deflecting the body of the adult back with the child firmly pressed to the chest. Increases the angle of inclination of the child’s hips.


The exercise is performed with VT + and VT ++ after mastering 1.2 and 1.3. Start the deviation from 30 degrees, gradually increasing to 45 and more. Achieve independent fixation of the head for at least two minutes, we attract the attention of the child from the front bottom.





The first variant of «monkey» introduces the child the need to hold their body with their hand by grabbing. Offer forefinger or thumbs for grip, changing sides as it weakens. Supporting a child with their back on the hips of an adult becomes mobile, forcing it to strain harder in attempts to prevent their fall.



The continuation of the first variant. Remove the support from under the back, gradually increase the angle of inclination.

Holding the child on the «monkey» position is available to mastering after the previous exercises are done successfully. To capture and hold the child is first offered a thumb, then the child masters an independent grip on clothes. Exercise is effective only with a constant deviation of the child back.



The suggested variants greatly facilitate the holding of the head in a position on belly, while improving the supporting function of the hands. Elbows lying on the surface should be spread apart.
Sloth». Hold (carry), changing arms, stroking (massaging) the back. The head is upper than the pelvis.

Lying on a belly with a roller under the chest.

Lying on a belly with an arm under the chest.

Lying on the chest of an adult.

Stimulation of turns from back to belly is necessary only after the confident mastering of previous exercises and the absence of independent turns. Performed by the hand and foot. It is important to stimulate the child’s efforts in the right direction, and not to carry out a turn for them.














The block of the turns from back to belly occurs by monitoring the constant dilution of the elbows to the sides. It is important to completely exclude the possibility of such turns.
Pulling the child's arms to the sides, we swing the child.


Playing with a child with a fixation of the pelvis by the leg.

Fix the child’s hands with a non-stretchable fabric (disposable diaper) to exclude the possibility of stretching the arm forward or placing it under you.




Using balls for table tennis and rubber bands create obstacles for turns and (or) make lying on their back uncomfortable.

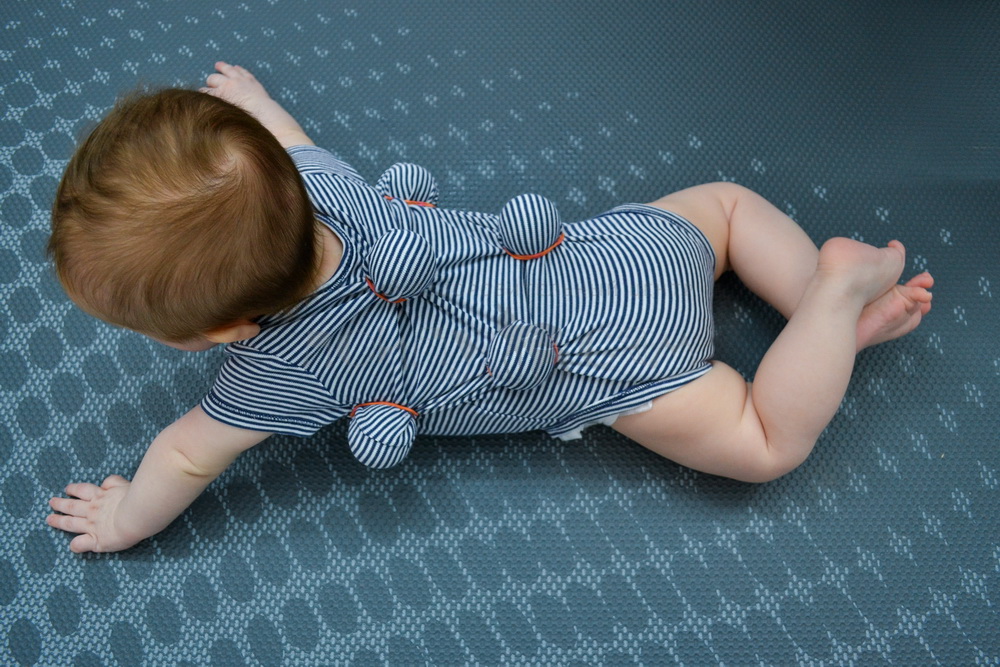
A piece of flexible dirt-collecting rug 10-12 cm wide and equal to 80 percent of the circumference of the chest is placed under the shirt with thorns inward across the body closer to the armpits.



On a tightly fixed and well-knit cap that covers the head, we sew the elements of the Kuznetsov applicator on the outside, but with thorns inward according to the scheme.


Any kind of fixation of the child on belly with the help of the adult's arms and legs, as well as with the help of a tie, should completely deprive the child of the opportunity to turn over onto their back.
The use of a «hedgehog», a thorn and a cap allow a turn, but at the same time, they should form a persistent negative attitude to this process and to the very fact of lying on back.
Independent activity (set of movements without outside participation)
VT + (vertical test is positive)
Lying on a back (mainly). Lying on a belly.
VT- (vertical test is negative)
Lying on a back with a centering of the head and bringing the chin to the chest. Feet may be raised.
Lying on belly is permissible for a long time only during sleep and rest with a lying head, briefly with a raised head without stimulation of its holding and elbows to the sides.

Position in the arms of an adult
VT+ (vertical test is positive)
doing a «sloth» exercise (1.6.1);

exercise 1.3 without a roller;

slanting positions (adult stands, sits), SLING.

VT- (vertical test is negative)
Exclude carrying in your arms with the body tilted forward.
carrying in the «sloth» position;

exercise 1.3 with a roller.

Sitting
IT IS CONTRAINDICATED IN ANY FORM
Positions for feeding
Lying position, half-lying, except for tipping and turning the head and twisting the body.


Positions for bathing
VT + (vertical test is positive)
Mostly on the back.
VT- (vertical test is negative)
Only on the back with the support of the nape.
Diving, the use of laps for swimming (on the neck) are excluded.
 Блог Муромова Д.С.
Блог Муромова Д.С.
 8 (917) 113-02-40
8 (917) 113-02-40
 Samara, Lenin Avenue, 3
Samara, Lenin Avenue, 3 
